


Graphics by Sahana Prabhu.


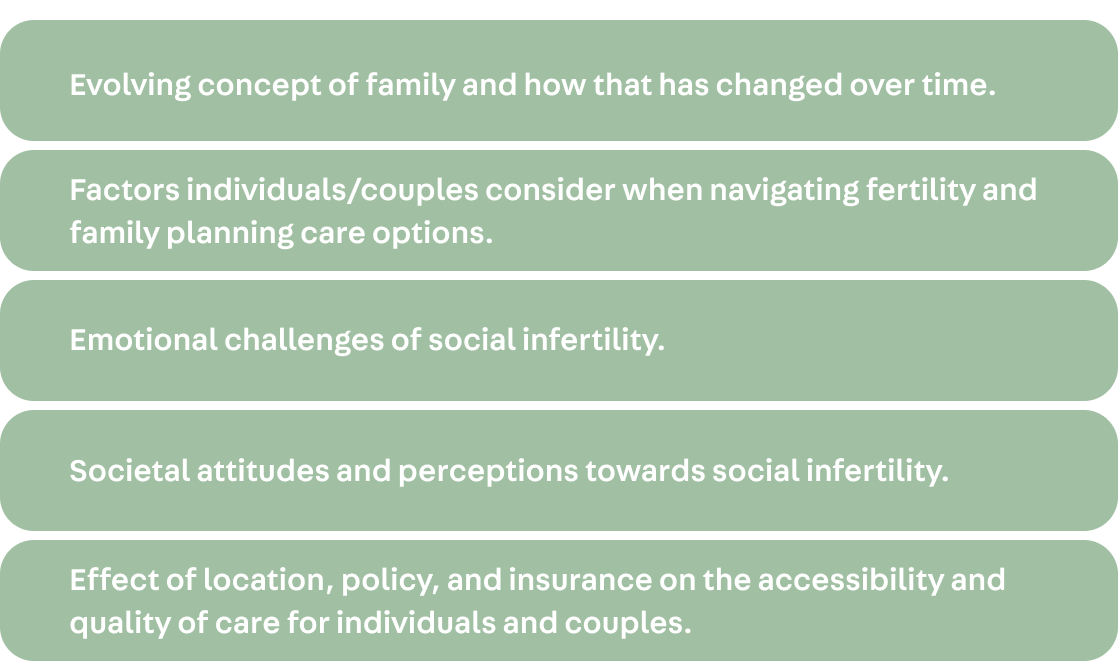
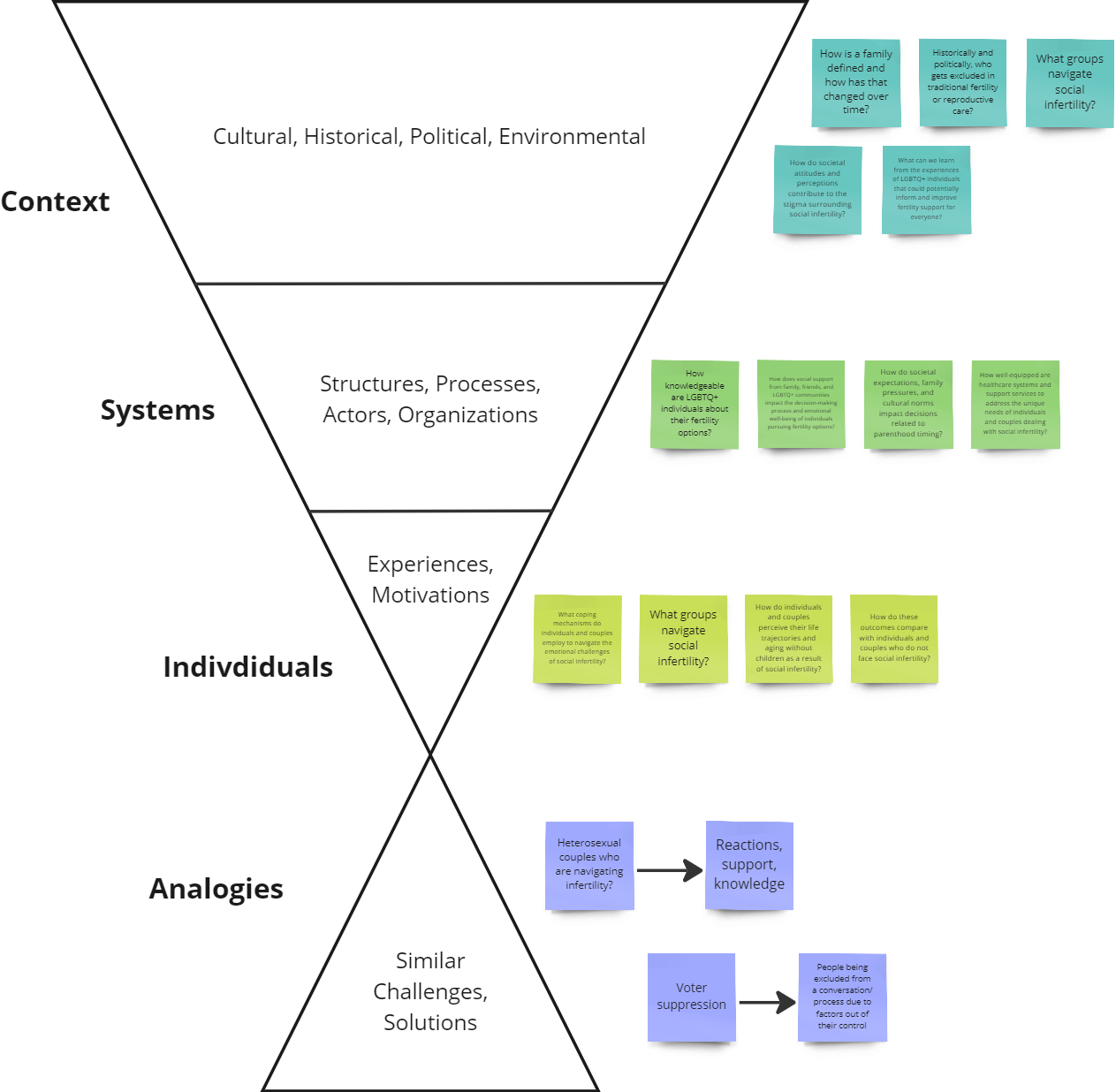
Setting our research goal: who is affected, what are the known challenges, when does this occur, and in what context does this problem show up?
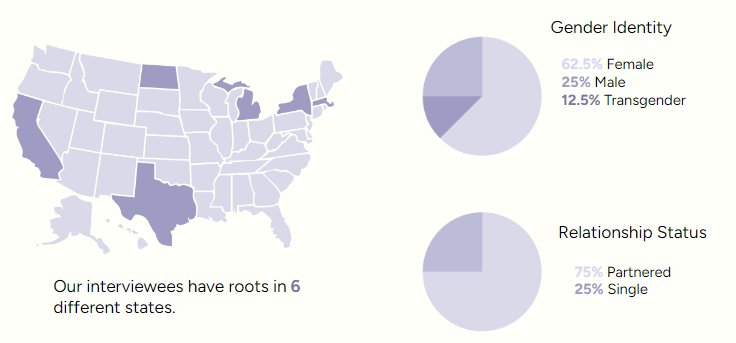
Participant overview.
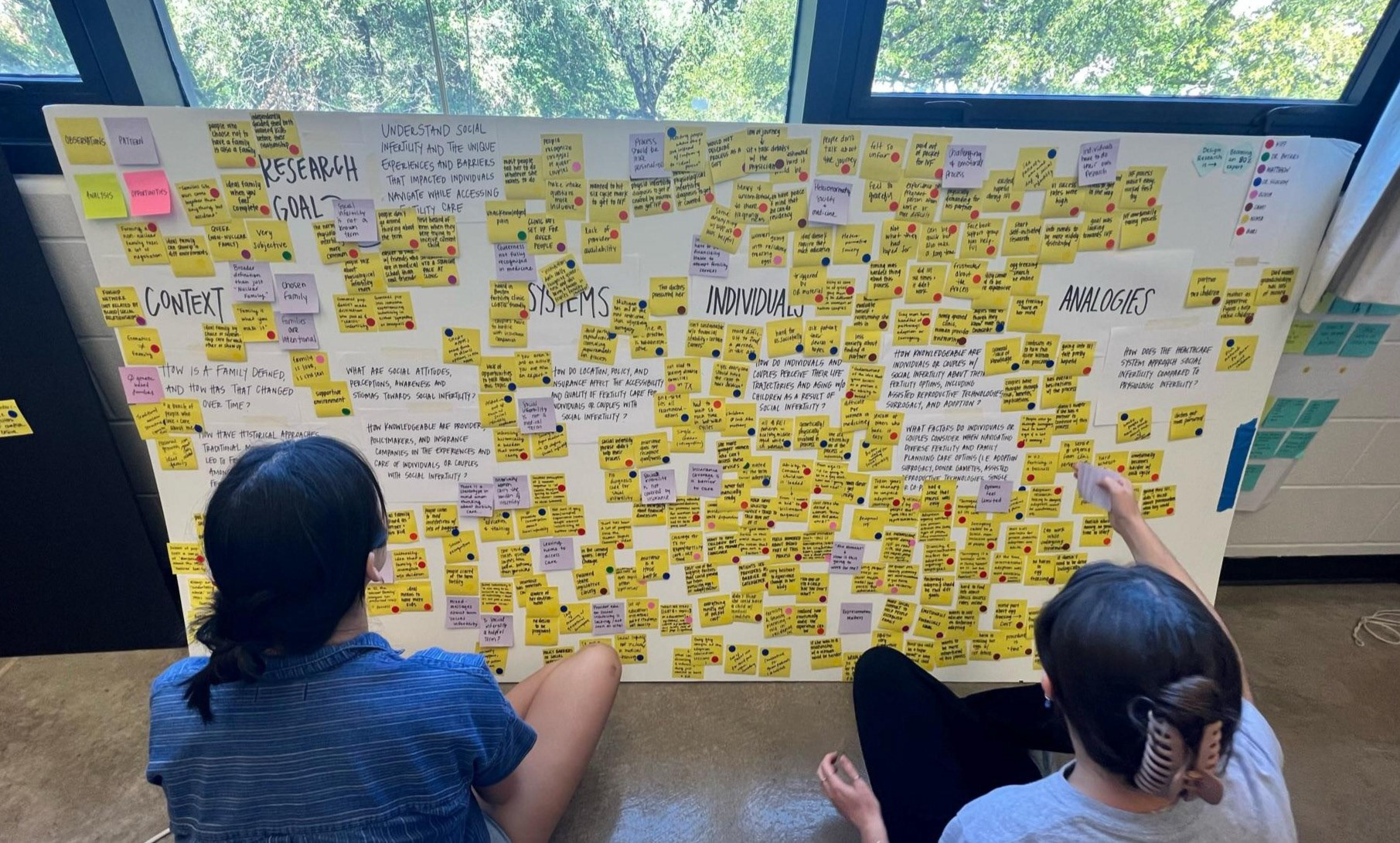
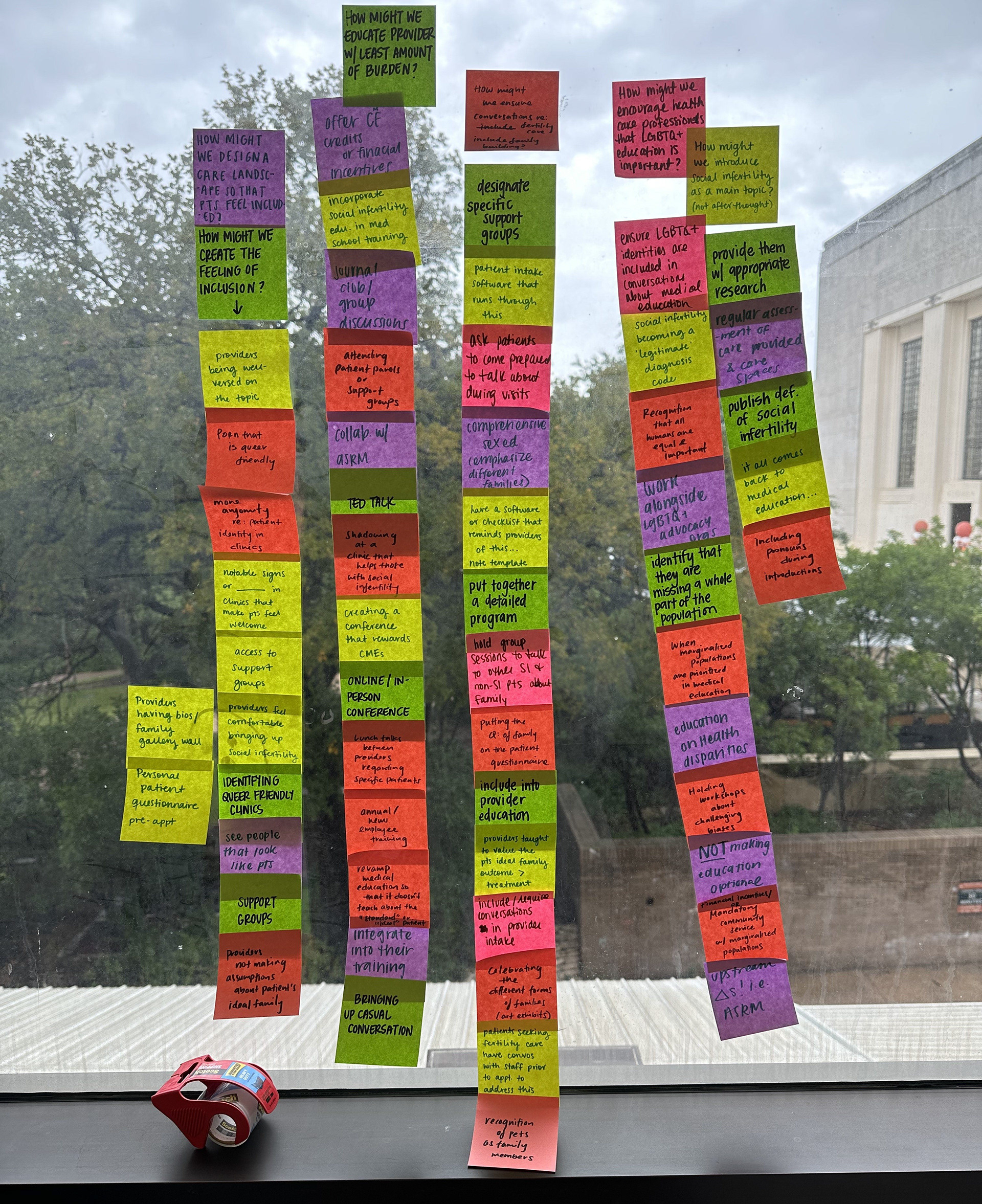
Early stages of synthesis. Sorting observations (yellow) into patterns (purple).

A small cross-cut of our synthesis process.
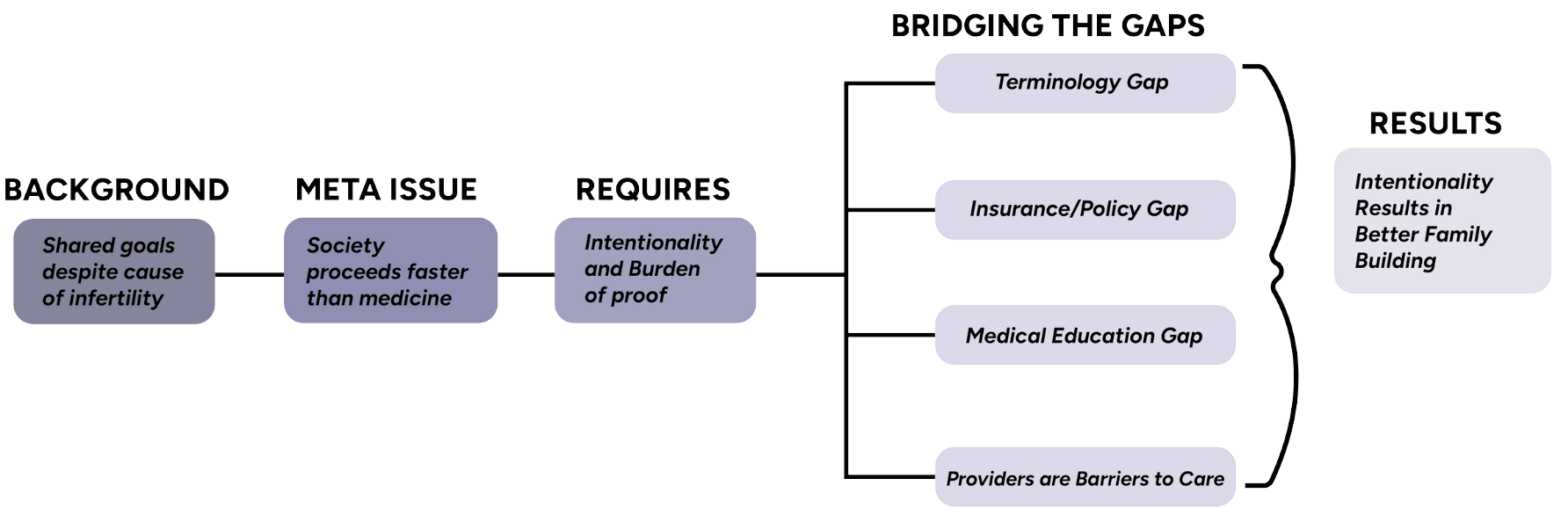
Our insight framework.
Those navigating social and physiological infertility share a fundamental goal— the desire to build a family. Regardless of the diverse roots of their infertility, those navigating infertility share commonalities and unity in their journey.
However, the larger issue is that society moves faster than medicine. Medicine is rooted in evidence, and change relies on a high burden of proof.

Because medicine is constantly playing catch-up to society, those navigating the social infertility care landscape have to be more intentional when building families while also often bearing the burden of proving they are physiologically infertile to gain access to care.

Barriers patients and their families have to overcome include: stigma with terminology, fitting the clinical definition of infertility to gain insurance coverage, lack of provider education, and patients often viewing providers as barriers to care.

Family building for those experiencing social infertility involves more intentionality— including researching methods and method availability, and challenging existing familial norms. Given the barriers these populations endure, they are more willing to build a non-nuclear family structure and very well-equipped to raise a family.

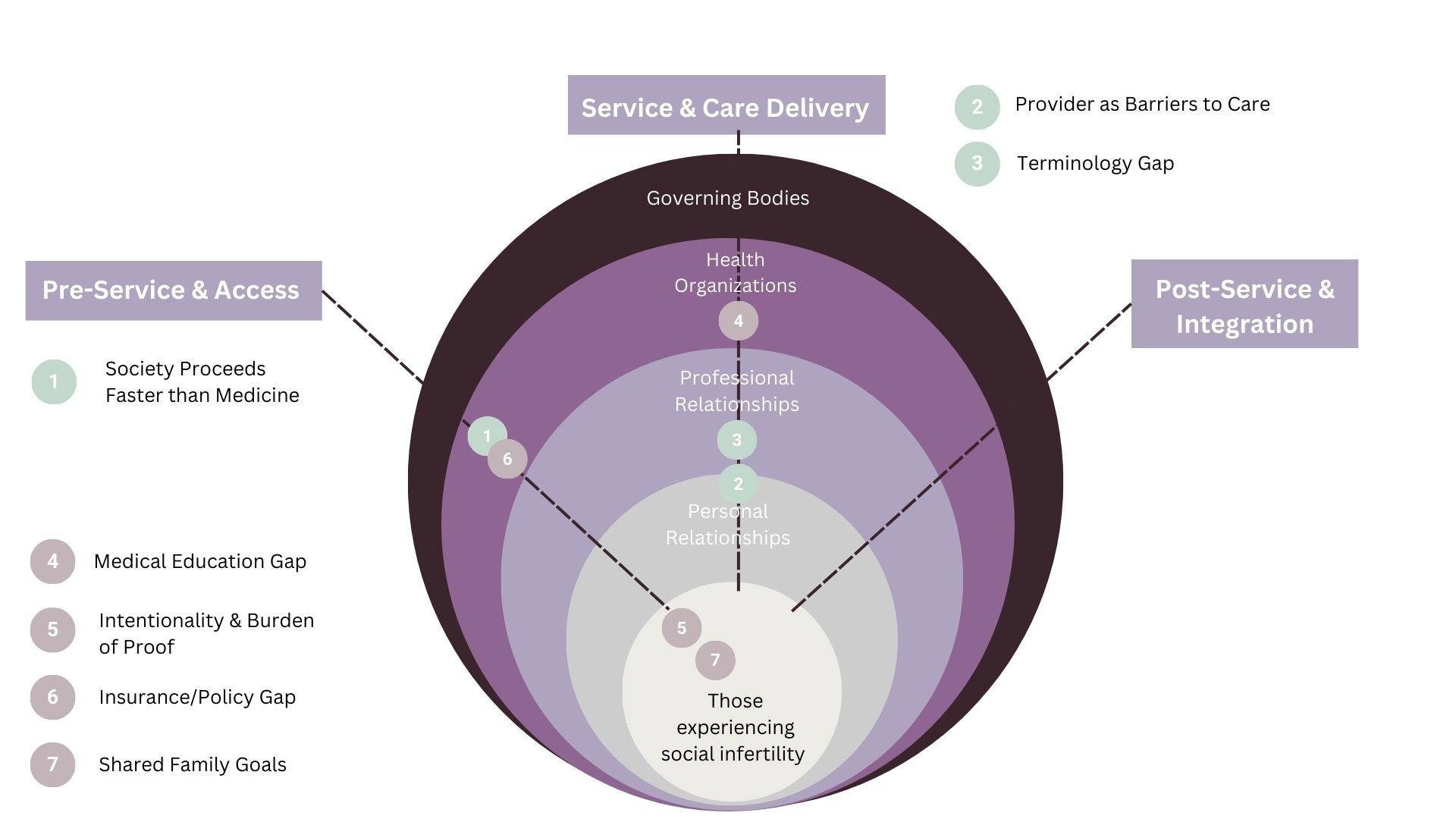
Ecosystem map with insights.
(2) seeking fertility care
(3) navigating care options
(4) receiving care
(5) navigating 'failure' and/or reevaluating care options.

(1) Society proceeds faster than medicine
(2) Providers as barriers to care
(3) Terminology gap.

Outcome-driven insight prioritization.
Rapid-fire ideation!
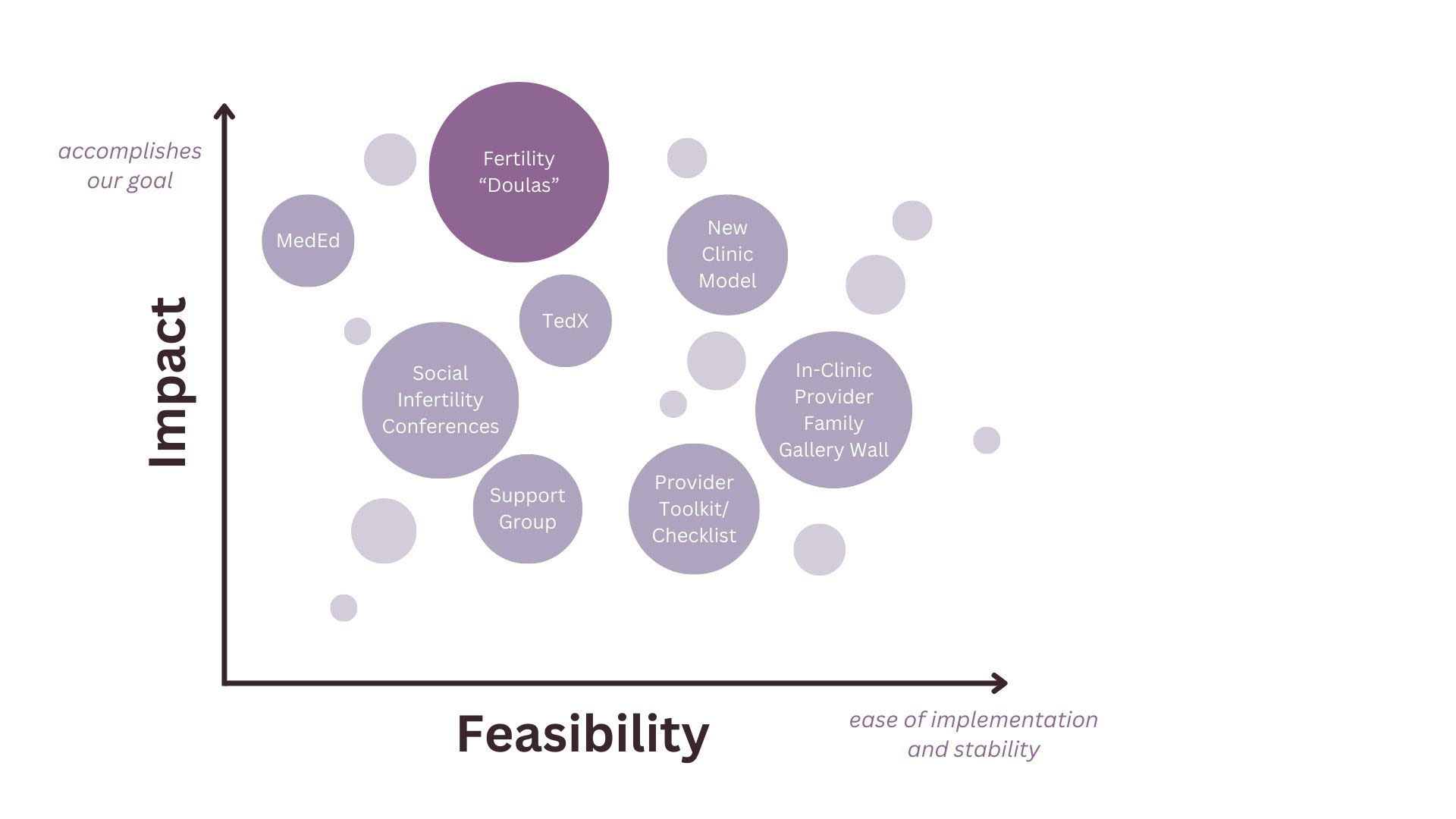
Impact and feasibility matrix.

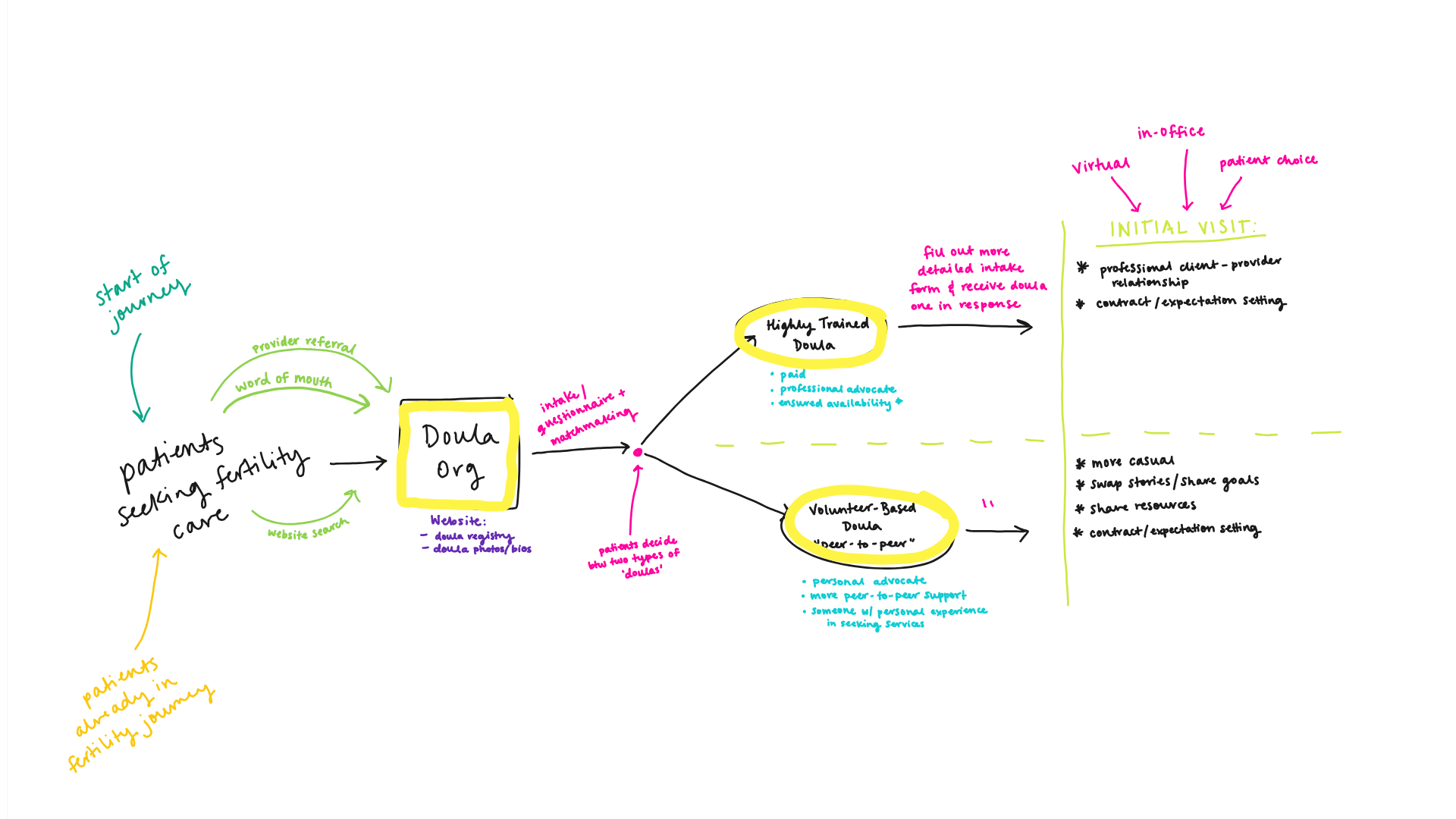
Early stages of Embr brainstorming. Sketched on Miro.
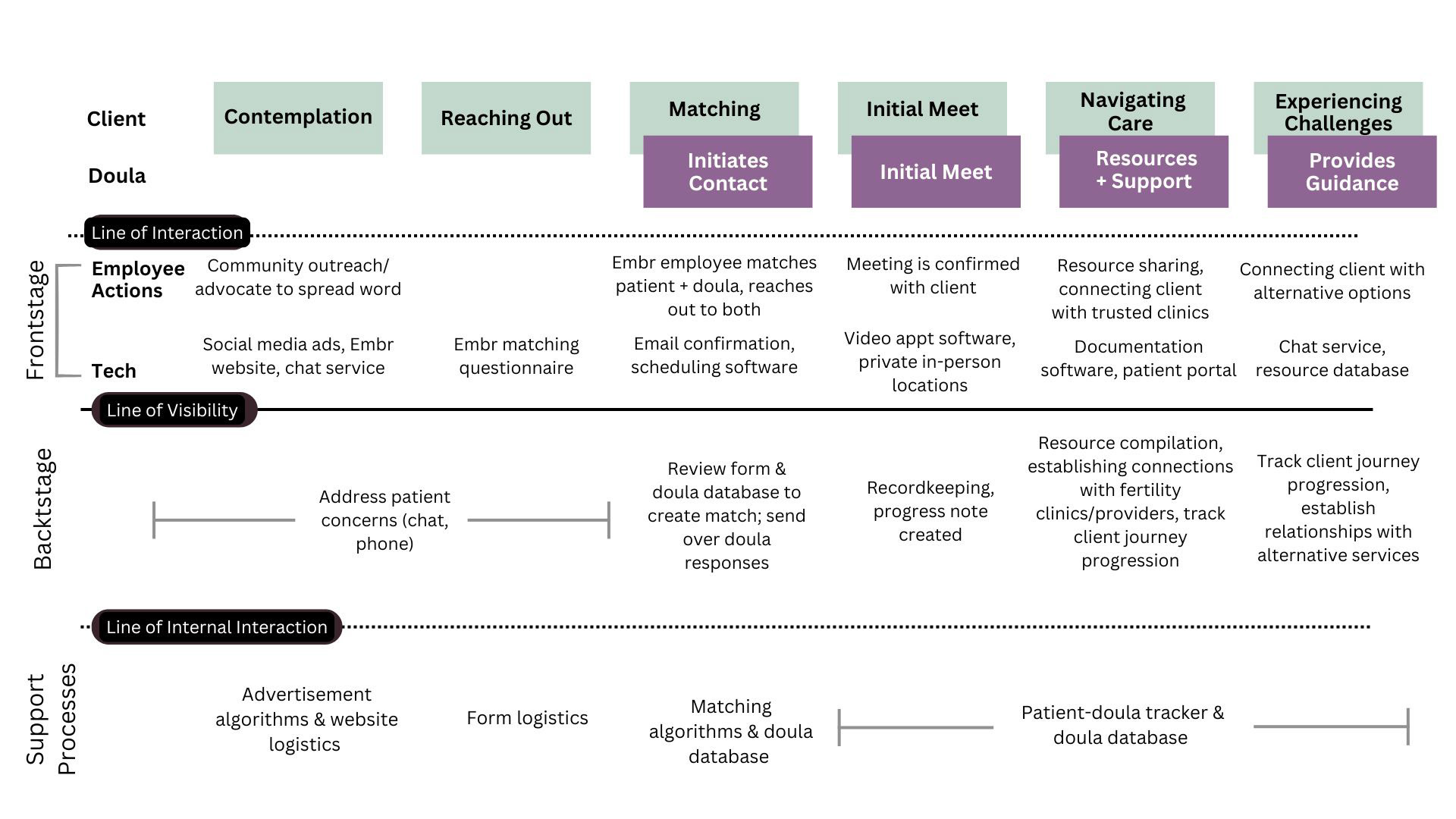
Service blueprint created on Miro.

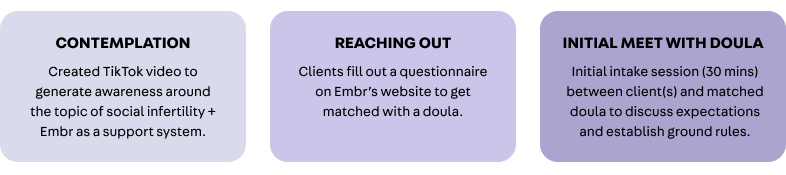
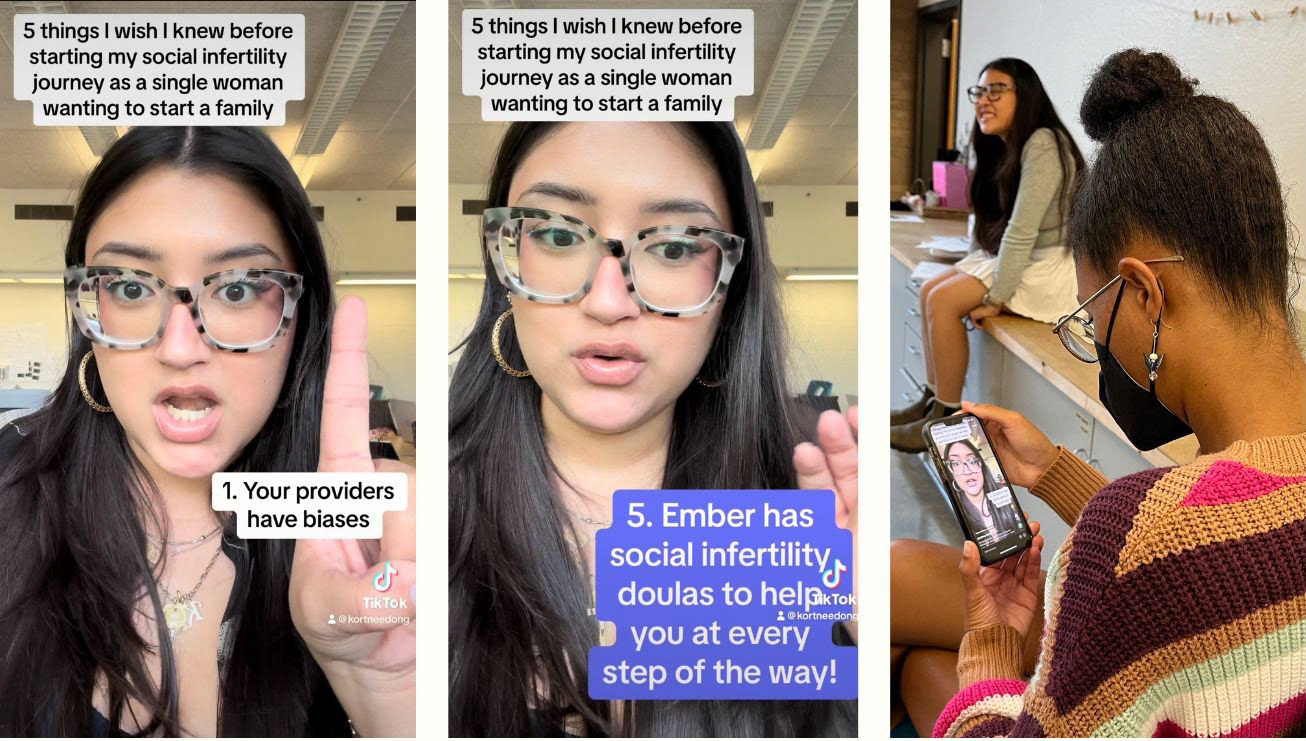
Prototypers watched a TikTok influencer share her experience with social infertility and Embr.
A hand-drawn wireframe of the Embr questionnaire prospective clients would complete before accessing services.

Prototyping a 30 minute doula intake appointment for a new client.

A shared, evolving document outlining ground rules involving communication, boundaries, conflict resolution strategies, and feedback.

Presenting at UT Austin's 2024 Interprofessional Health Showcase.

Design in Health Team. From left to right: Laura Long, Courtney Duong, Sahana Prabhu, Karen Jimenez, Alice Liu


