

01. OVERVIEW
PERSONAL TAKEAWAYS + REFLECTIONS:
02. INTRODUCTION
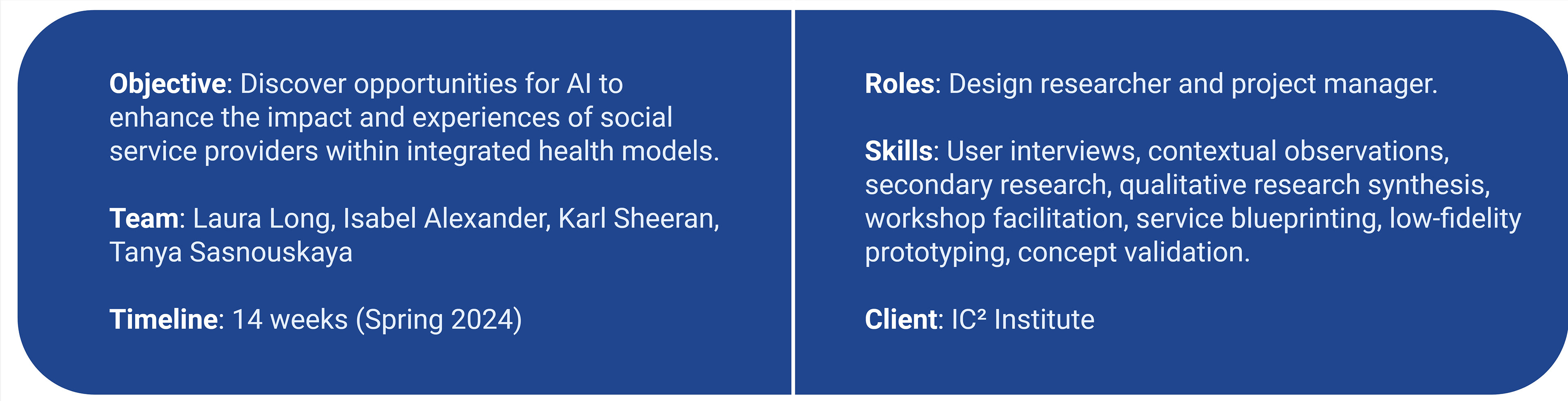
While AI is currently being implemented in many corners of healthcare, our research highlights social service providers (SSPs)—specifically, social workers, community health workers, and peer support specialists—whose perceptions of and need for AI have been relatively overlooked thus far.
In partnership with the IC2 Institute, we conducted research to explore the key priorities, challenges, and experiences of social service providers— identifying opportunities for thoughtful technological integration into their existing workflows.
WHAT WE SET OUT TO LEARN:

Ultimately, we wanted to imagine a future in which a greater diversity of healthcare professionals, and the patients the serve, can benefit from the intentional integration of AI. In parallel, unearthing and addressing the concerns that these technologies may provoke.
PLANNING:
To prepare for our research, we hosted a client kick-off meeting where we ran through introductions, project overview and scope, success criteria, research expectations, and communication preferences. We also wanted to foster a collaborative relationship with our client and decided to host weekly check-ins where we could update on our progress and next steps, while allowing for open discussion and questions from both teams.
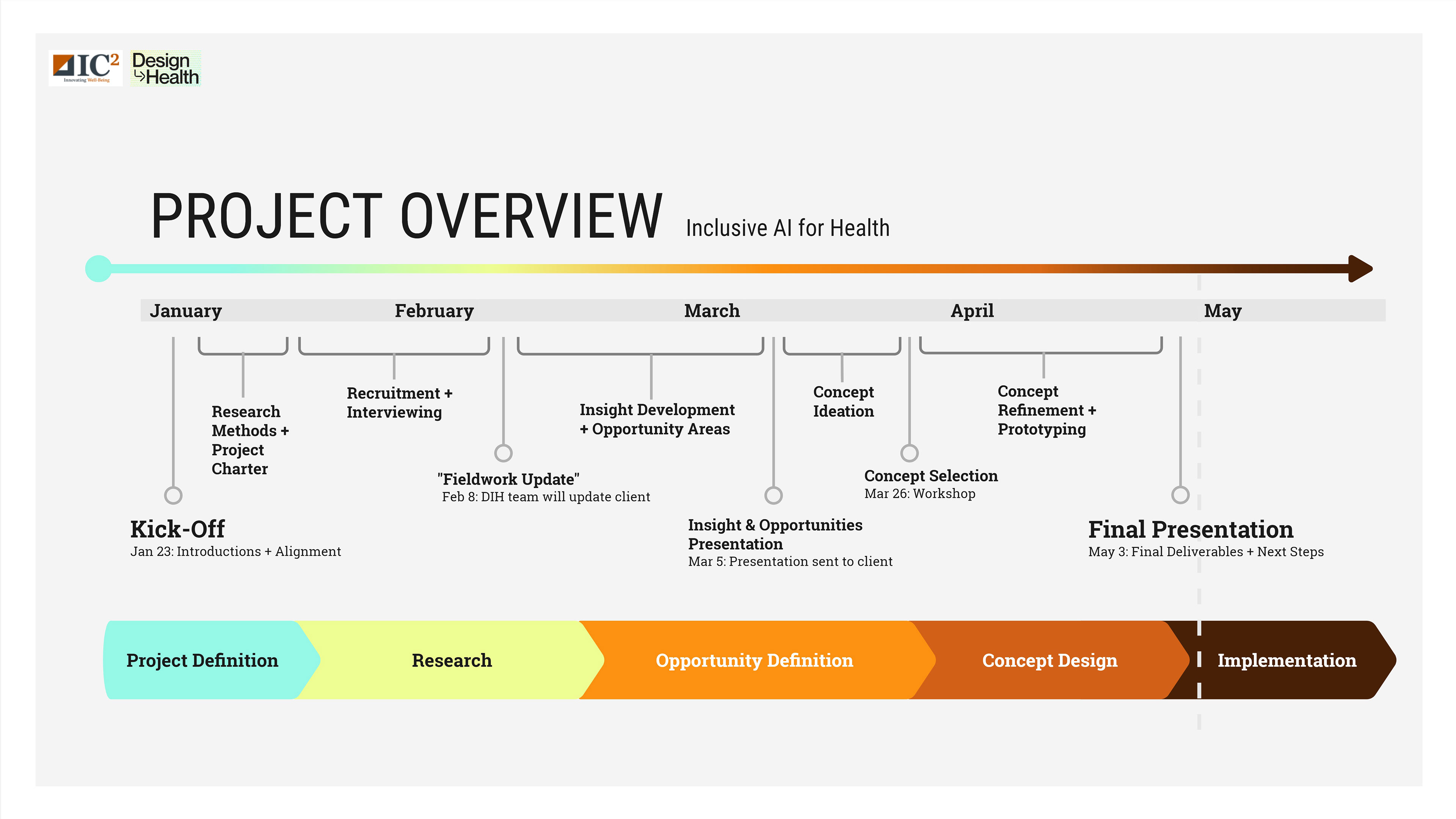
Project overview timeline - I created this on Miro.
During the kick-off meeting, we:
• Clarified the project's emphasis on experimentation/exploration of de novo AI solutions, informed by the experiences of these SSPs.
• Discussed high priority research focus: identification of barriers to AI adoption, specific to research population.
• Discussed recruitment, targeting a sample of 15 participants with diverse roles in healthcare.
• Clarified the project's emphasis on experimentation/exploration of de novo AI solutions, informed by the experiences of these SSPs.
• Discussed high priority research focus: identification of barriers to AI adoption, specific to research population.
• Discussed recruitment, targeting a sample of 15 participants with diverse roles in healthcare.
03. RESEARCH
RESEARCH GOAL:

METHODOLOGIES:

To guide our research questions and interview guides, we created a conceptual framework highlighting the interrelated components of healthcare provider workflows: patient care, interdisciplinary collaboration, and administrative tasks. We also probed on factors that might influence AI adoption at individual, organizational, and societal levels.
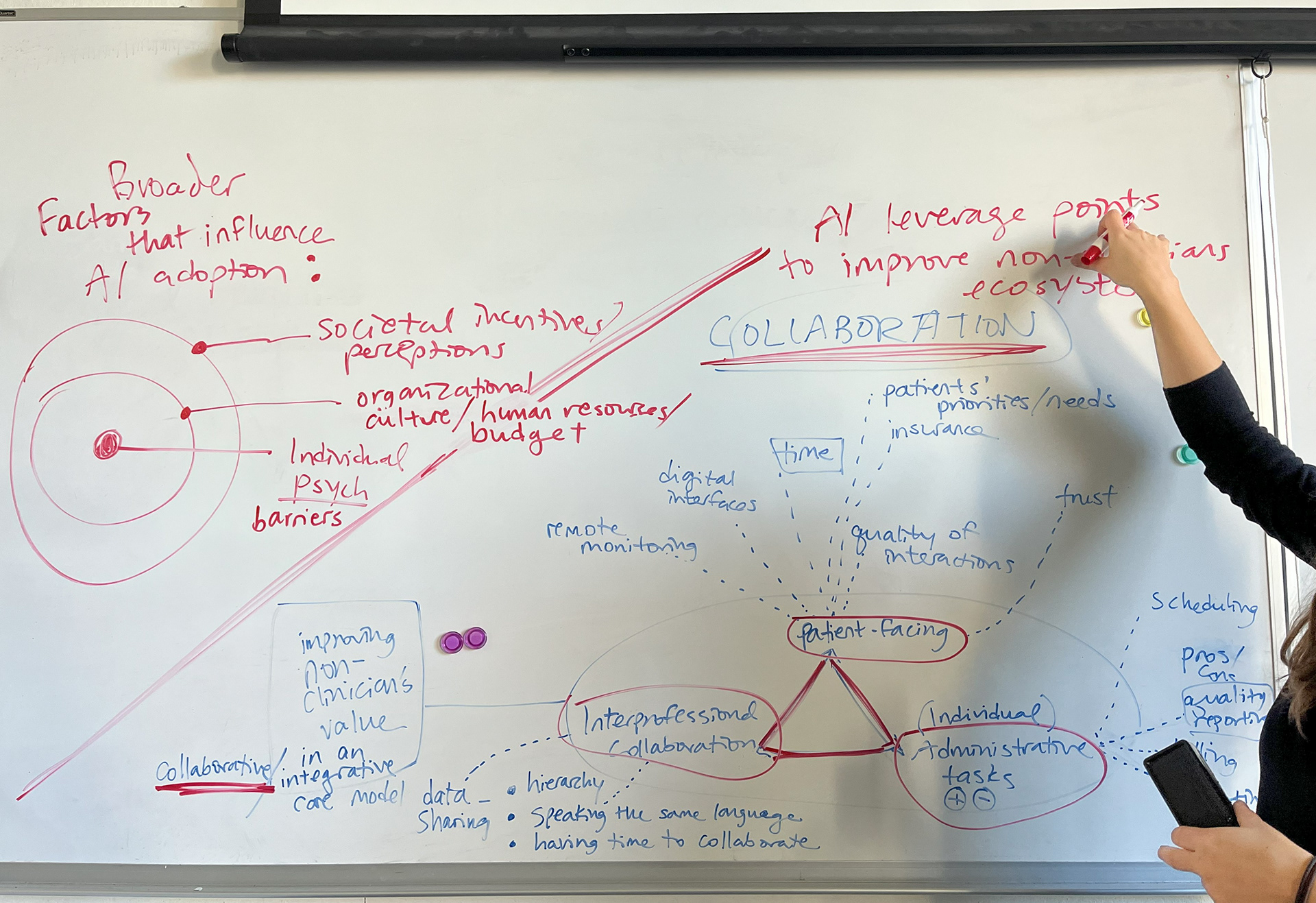
Early research framework brainstorming!
INTERVIEWS
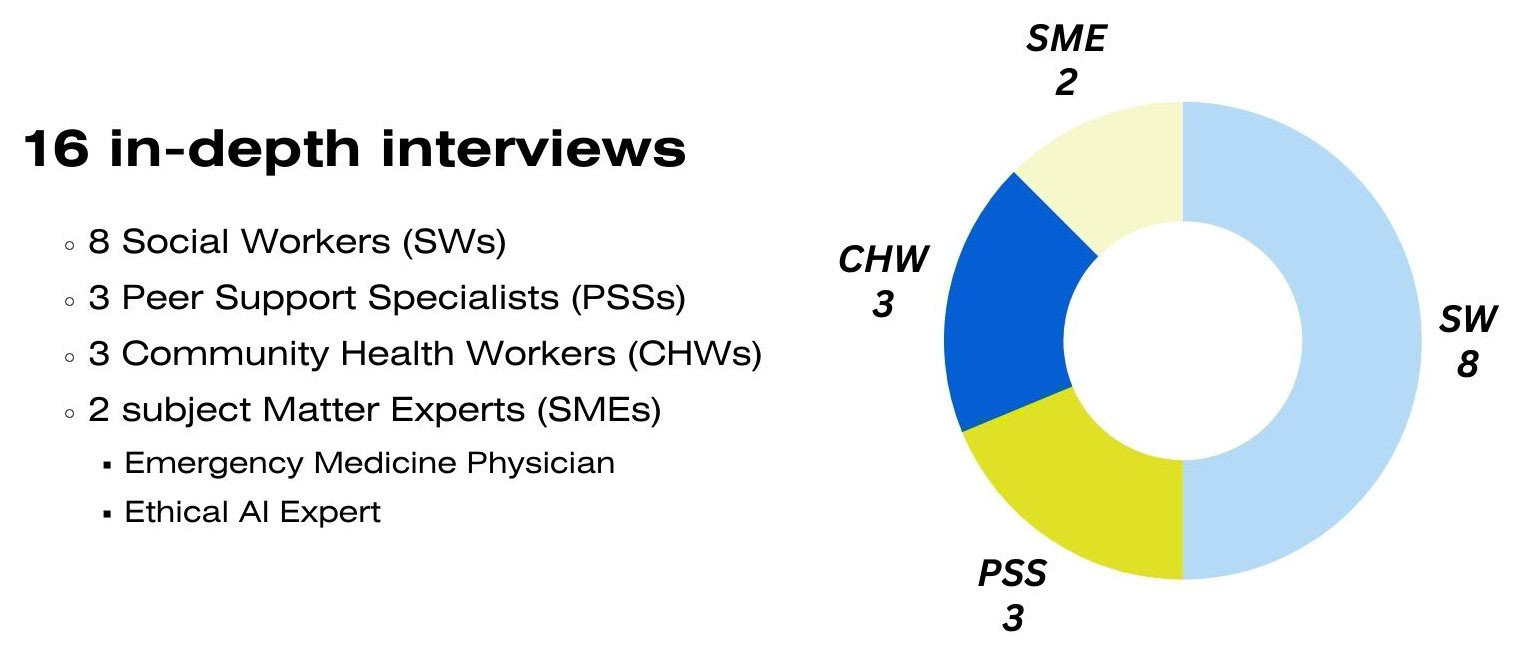
We conducted 16 semi-structured interviews with social workers, peer support specialists, community health workers, an ethical AI expert + foresight practitioner, and an emergency physician.
We chose to conduct both in-person and virtual semi-structured interviews to (1) fit into these practitioners' busy schedules in a way that was accessible and of choice, and (2) balance consistency (having a set interview guide) with the flexibility to explore individual experiences and nuanced needs.
INTERCEPTS
In addition to our structured interviews, we attended a local community health worker social event.
We were able to speak to 12 attendees and used this opportunity to distribute QR codes linked to a survey with a condensed set of interview questions. While unsuccessful in gathering responses from the online survey, we were fortunate to have many meaningful conversations on the landscape of community health work and the hopes and fears of AI integration into their work.

CHW social event in Austin, TX.
CONTEXTUAL INQUIRY
I was able to participate in an 8-hour solo ride-along with the Austin Community Health Paramedic (CHP) program— a unique EMS model centered around proactively managing healthcare needs for unhoused and underserved populations in Travis County, TX.
Shadowing CHPs provided a complimentary perspective to our interviews as they often interacted closely with the social service providers within our scope. I was able to witness the critical and collaborative role SSPs can have in emergency settings and health crises.

Austin EMS ride-along.
ANALOGOUS RESEARCH
IC² Institute hosted our team for a prototype demonstration and end user walkthrough of an AI-based technology they are developing to offer real-time emotion data tracking to behavioral health providers and their patients.
We aimed to get a better understanding of the logistics behind creating this technology, as well as take in feedback from the end users (team of doctors, nurses, case managers, administrative professionals) to identify transferrable insights to our own research.
We aimed to get a better understanding of the logistics behind creating this technology, as well as take in feedback from the end users (team of doctors, nurses, case managers, administrative professionals) to identify transferrable insights to our own research.

The IC2 and Design in Health teams.
04. SYNTHESIS + INSIGHTS
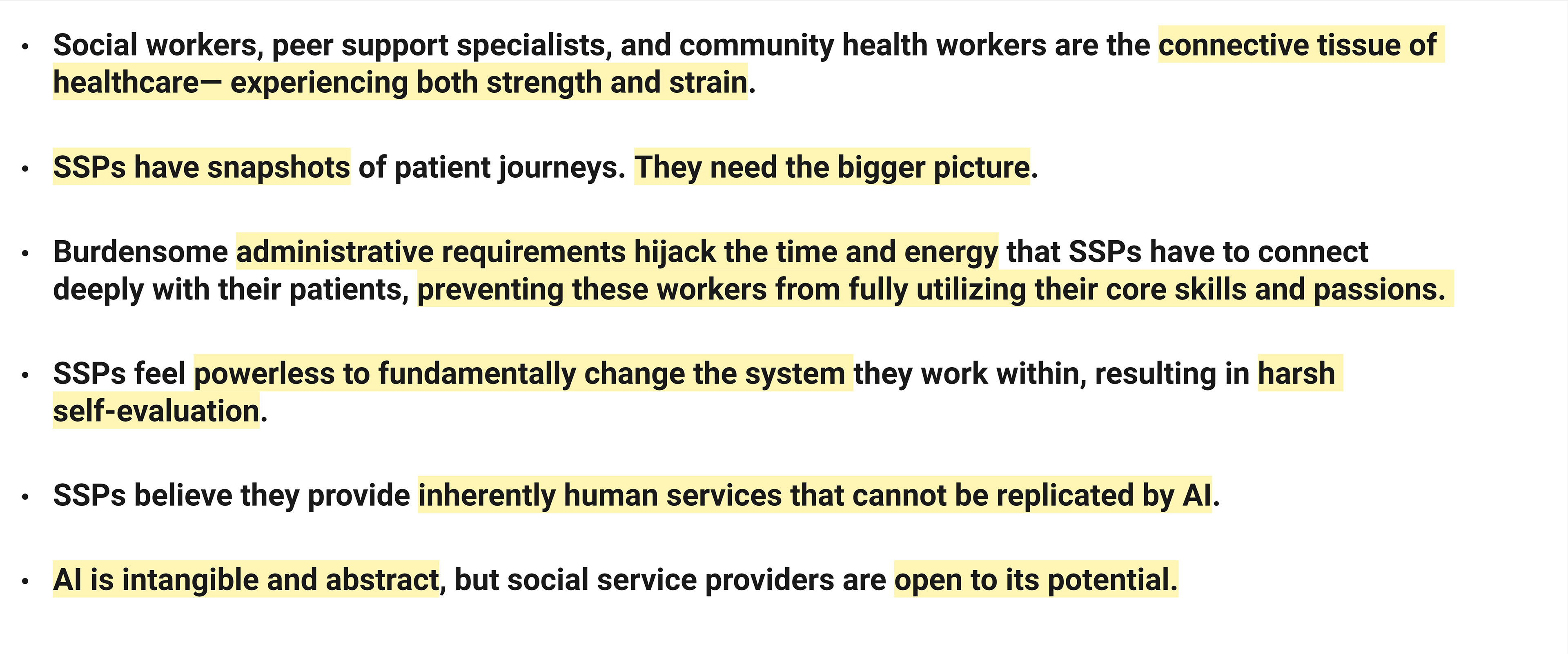
After completing our research, we began synthesis— moving from research observations to our final nine insights. We primarily utilized a manual thematic analysis approach—immersing ourselves in the data (interview transcripts, notes, and intercept observations) to identify patterns in behaviors, perceptions, and experiences. Tools used in this process included Miro, Google Suite, Zoom, and analog methods such as sticky notes and poster boards
Each uncovered insight highlights the interconnected experiences and pain points of social service providers, uncovering meaningful opportunity areas for AI integration.
Our synthesis board, containing observations, patterns, analysis, and insights.
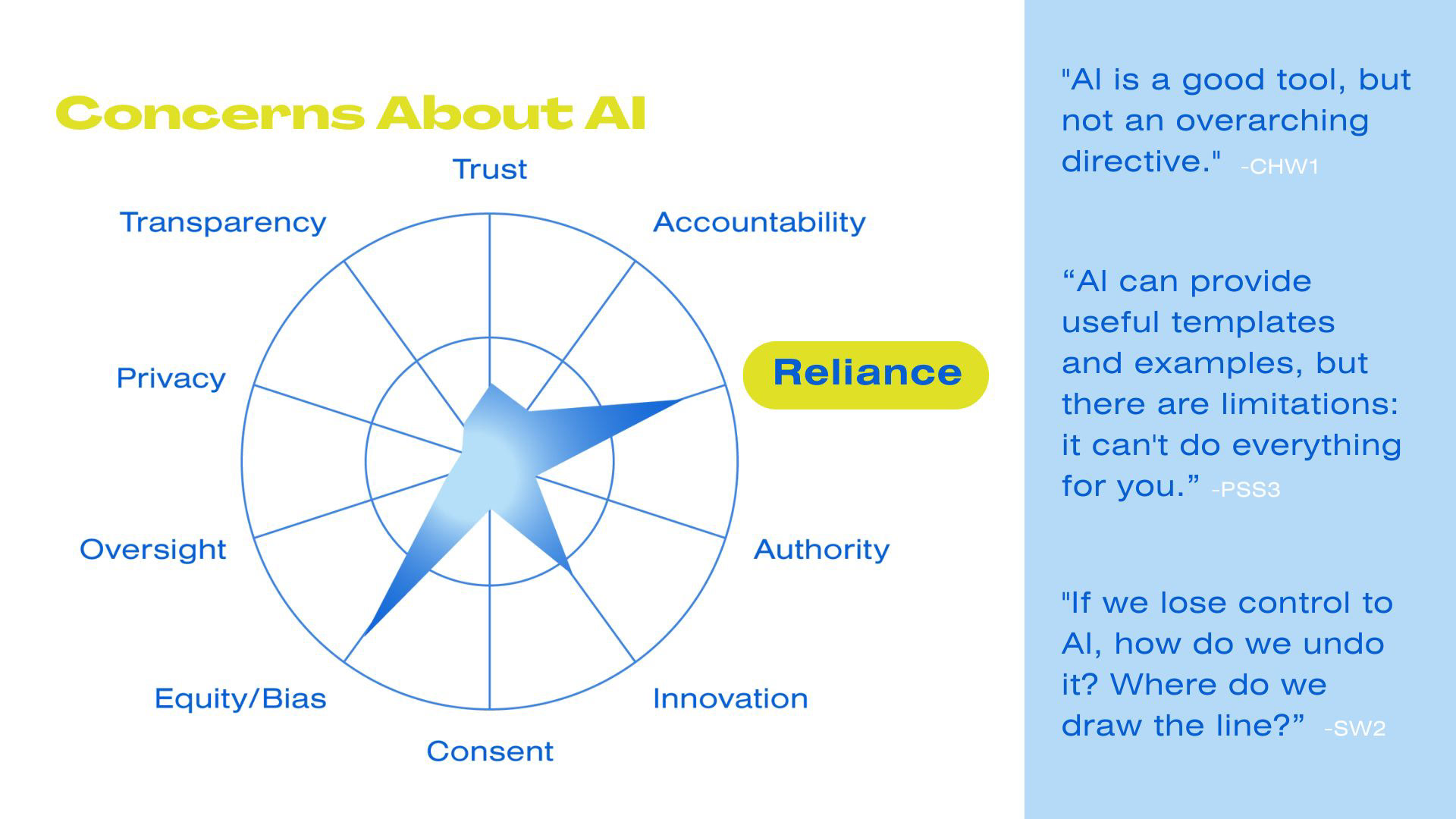
We created a section of our synthesis board centered around the AI concerns we were consistently hearing.

This let us quickly visualize the biggest concerns our research sample shared around AI being implemented in their workflows: reliance, innovation (AI being 'too innovative' for true adoption in social services), and equity/bias.
INSIGHTS: (selected sample)
05. DEFINITION + IDEATION
PERSONAS + OPPORTUNITY FRAMING:
To ensure that our design solutions were aligned with the real needs and preferences of our users, as well as tell the story of our research in a way that was empathetic and data-driven (not based on assumptions), we chose to explore creating personas. In general, these archetypes were helpful for asking the right questions, providing guidelines for design development, and identifying opportunity areas.
Example of a persona created to further guide our design process.
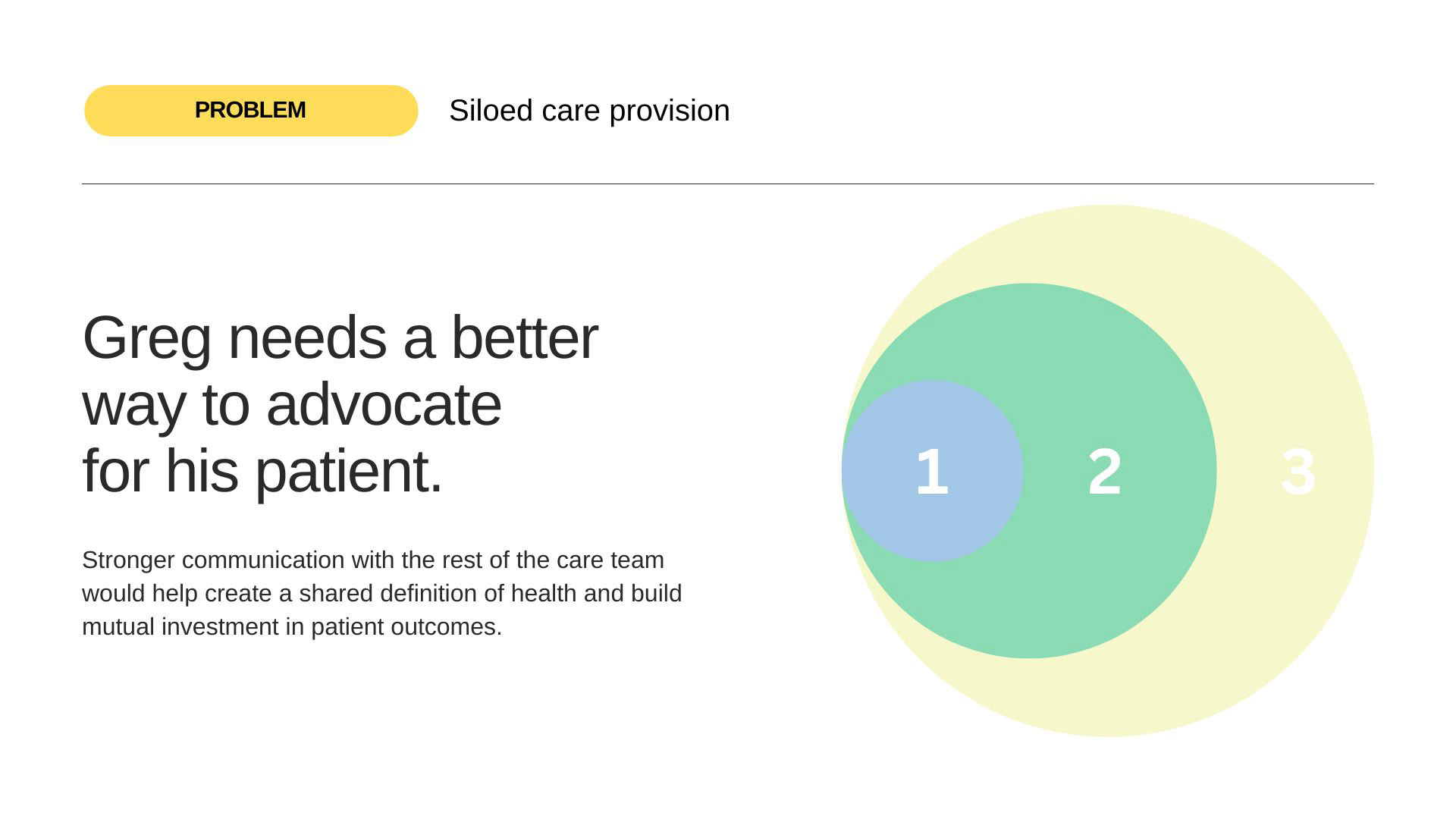
An opportunity area derived from our peer support specialist persona, Greg.
WORKSHOPPING:
To incorporate fresh perspectives into our work, we conducted a sprint-style card sort workshop with fellow classmates. My team chose to use this guided-but-flexible methodology to foster collaboration and encourage creativity in a low-tech, accessible manner. In preparation, we created two stacks of cards: a scenario/context card (touch points within an SSP's workflow, such as chart review or interdisciplinary team meetings) and a goal card (insights we were trying to address).
To incorporate fresh perspectives into our work, we conducted a sprint-style card sort workshop with fellow classmates. My team chose to use this guided-but-flexible methodology to foster collaboration and encourage creativity in a low-tech, accessible manner. In preparation, we created two stacks of cards: a scenario/context card (touch points within an SSP's workflow, such as chart review or interdisciplinary team meetings) and a goal card (insights we were trying to address).
I led teams through this workshop, instructing each to randomly pick one card from each stack and generate as many ideas in just a few minutes that would solve for those unique criteria. For example, "How can we empower social service providers to feel valued while summarizing and documenting a patient encounter?"
From there, we synthesized the ideas generated into six high-level solutions that we presented to our client. After discussing each idea, we had them rank the feasibility and impact of each proposition on a 2x2 matrix (pictured below).

Teams in ideation mode!

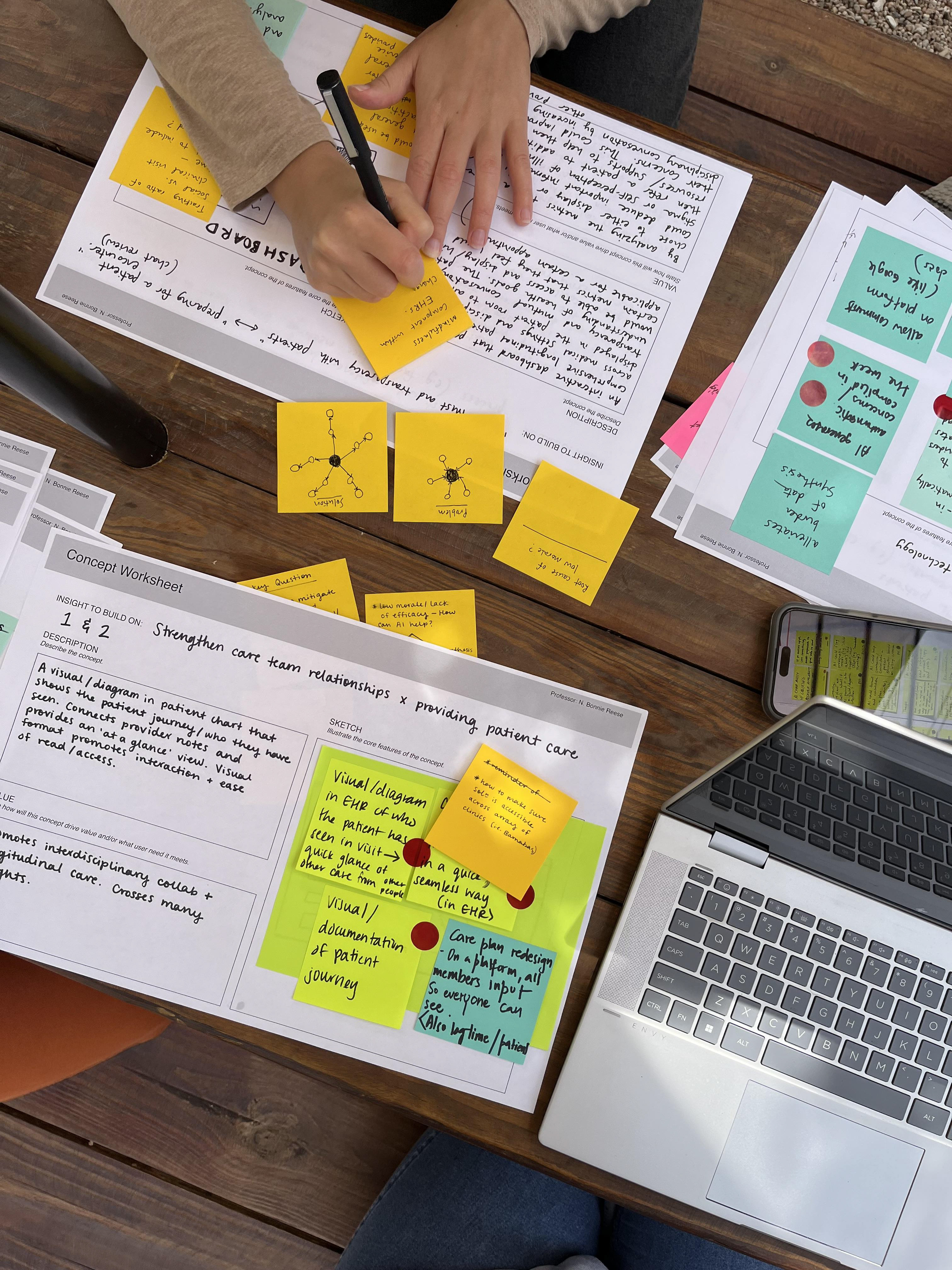
Card sort instructions and one working board that was then translated into a concept worksheet.
Team ideation at our favorite co-working (coffee) spot.
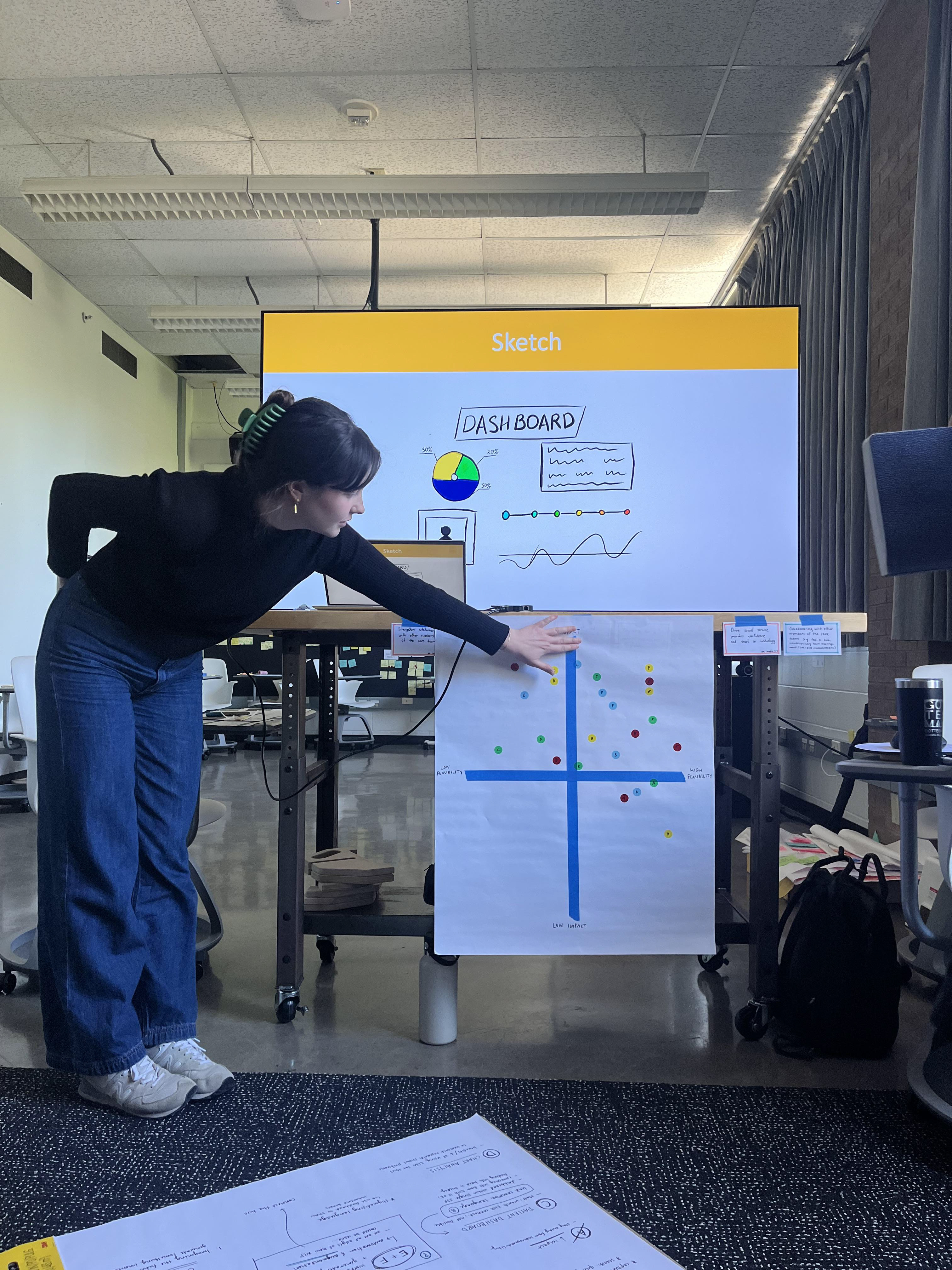
Presenting our initial concepts to our client for discussion and selection.
A PATH FORWARD:
We knew our concept needed to address three core areas:
(1) solving for immediate administration/documentation burden
(2) an efficient way to review a deeper, more holistic, bigger-picture view of the patient journey
(3) helping to increase SSP morale and reduce cognitive load— thereby reducing burnout.
(1) solving for immediate administration/documentation burden
(2) an efficient way to review a deeper, more holistic, bigger-picture view of the patient journey
(3) helping to increase SSP morale and reduce cognitive load— thereby reducing burnout.

Early concept brainstorming according to workshop input from our client. We knew we had lots of ideas (and more to come!) and would need to start narrowing down. I created this on Miro.
06. CONCEPT REFINEMENT
CO-DESIGN:
To test and validate our concept, we took it out into the field. We conducted co-design sessions with three social service providers— two social workers and one peer support specialist. These were in-person workshops conducted at each user's place of employment.
After presenting our preliminary concept to these stakeholders, we asked them to share what they considered to be the best and worst case scenarios for the three components of our proposed solution. This exercise helped us incite initial reactions, refine details and identify implementation considerations.
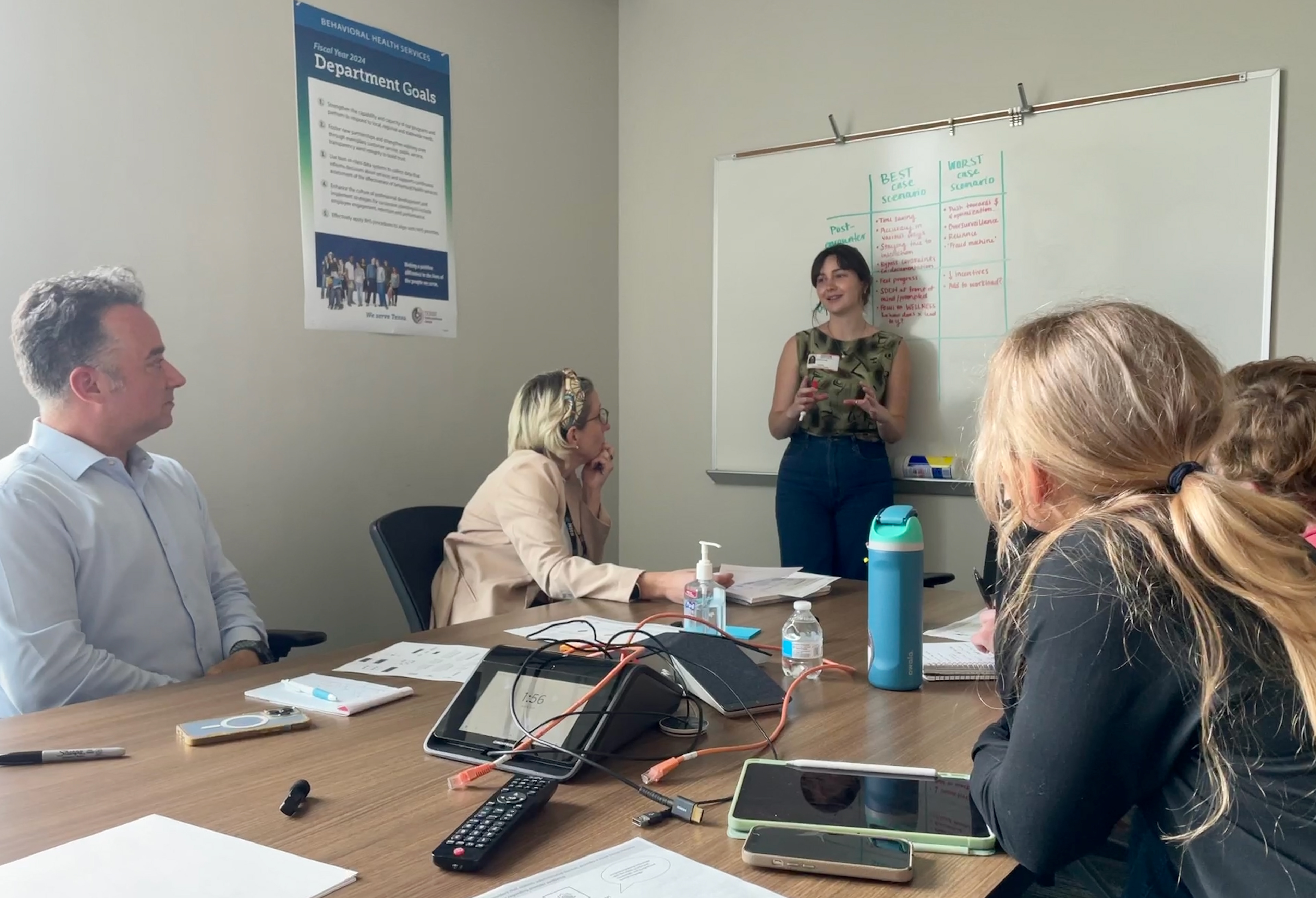
Leading a co-design/concept feedback session with two end users.
FURTHER INSPIRATION:
To strengthen our knowledge on AI in health— and what it means/will take to ensure AI is implemented ethically and equitably in this space— we attended the 2024 Health AI for All Conference at UT Austin.
It was a full day of learning from keynote presentations on the ethical, social, technical, clinical, and policy implications of deploying AI in historically vulnerable communities. We learned more about the specific capabilities of certain AI platforms, as well as the general best practices around co-design with relevant stakeholders.
2024 Health AI for All Conference, Austin, Tx.
07. PROTOTYPE
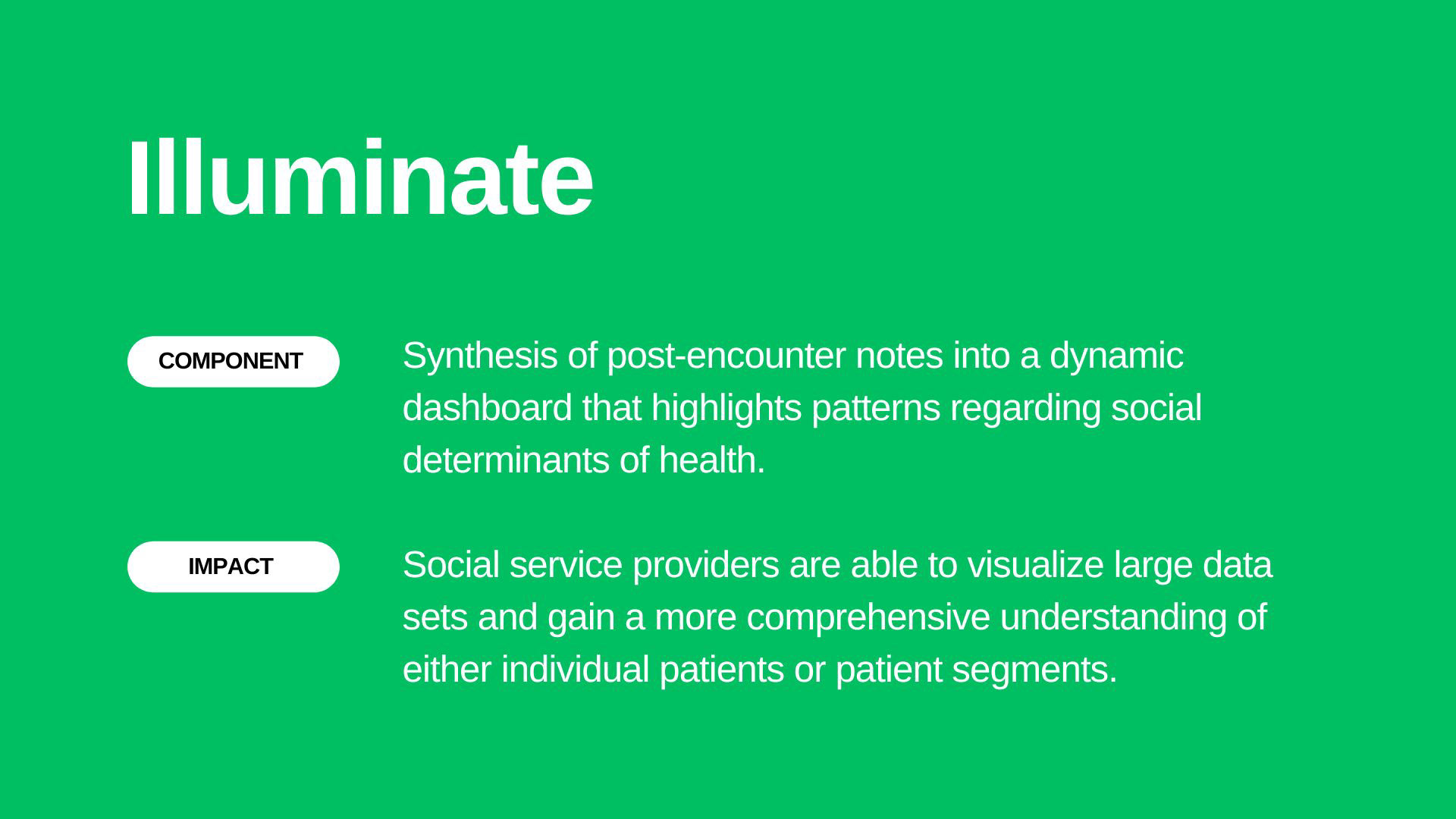
We proposed the customized implementation of Natural Language Processing (NLP) to streamline post-encounter documentation, illuminate patterns in longitudinal patient data, and engage other members of the care team around social determinants of health.
NLP is a machine-learning technology that helps organize, synthesize, and make sense of written and spoken data—often with more standardization and efficiency than manual human synthesis. In this project case, it can process relevant patient information (such as concerns, symptoms, questions, and dates) for SSPs.
We translated our personas and opportunity areas into three distinct design concepts for handoff. For each technological component, we created:
• High-level description of component and impact, grounded in research insights
• Further storytelling with each persona, illustrating how the component fits into their individual workflow
• A detailed summary page outlining the aspects of each component
• Mockups visualizing the potential design of each component
• High-level description of component and impact, grounded in research insights
• Further storytelling with each persona, illustrating how the component fits into their individual workflow
• A detailed summary page outlining the aspects of each component
• Mockups visualizing the potential design of each component

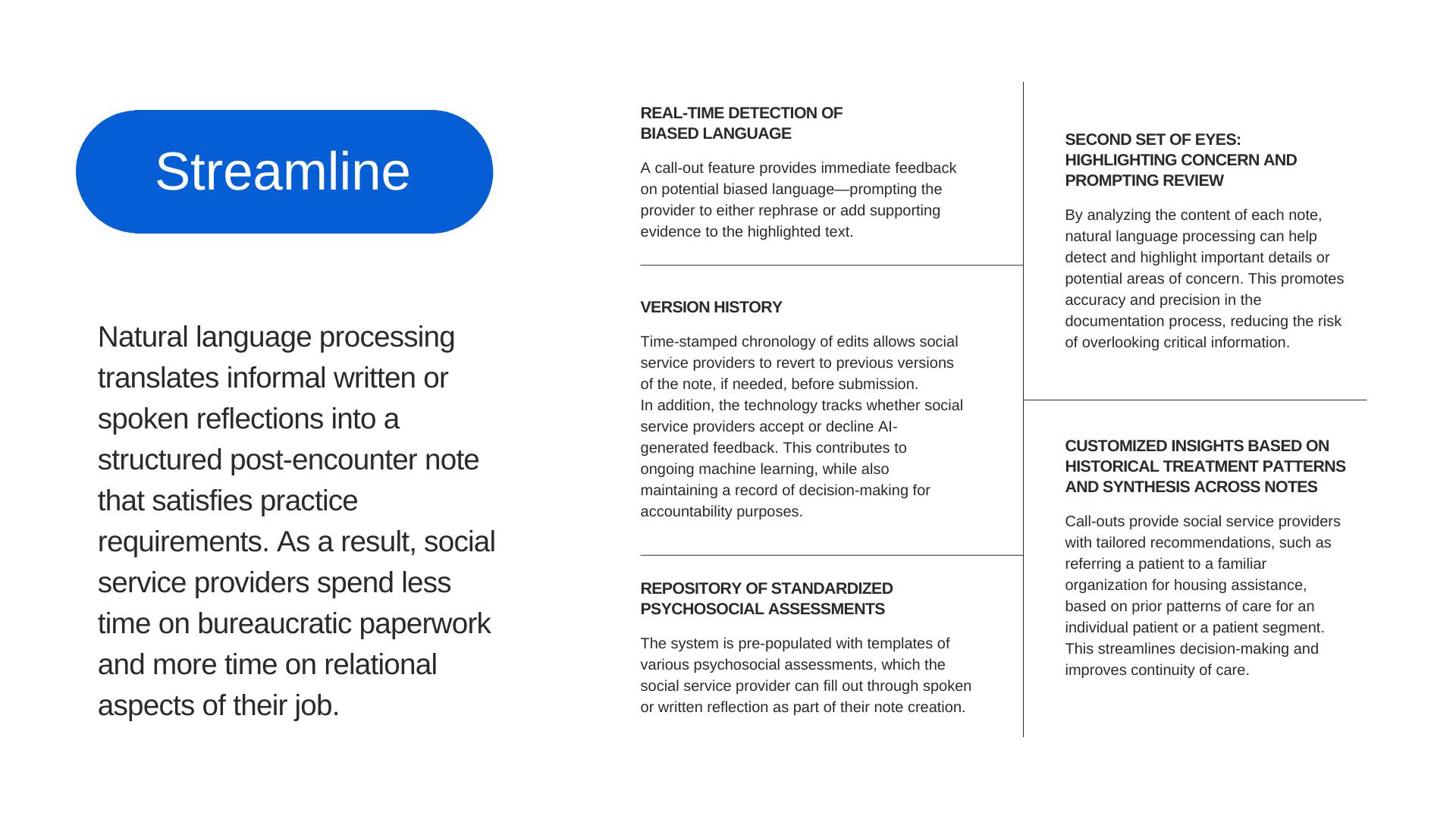
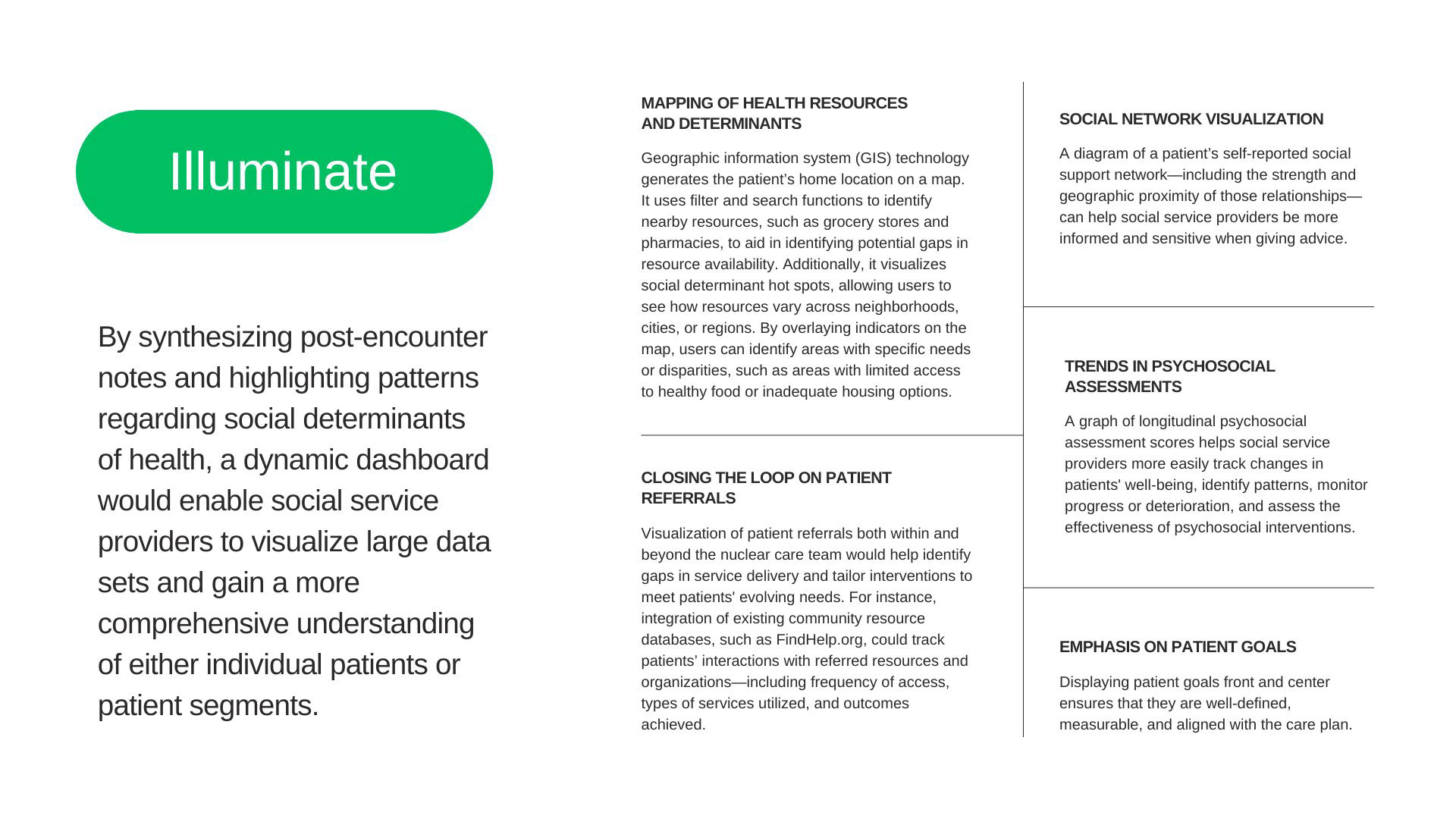
For the 'Streamline' component of our AI-assisted technology, we envisioned SSPs inputting informal written or verbal post-encounter reflections into a secure software platform that can connect to their EHR or records management system. These reflections are translated into a note that satisfies their individual practice requirements as well as analyzed for historical patterns, real-time detection of biased language, and tailored recommendations based on prior patterns of care or alerts.







IN SUMMARY:
While it feels ironic, artificial intelligence might just be the tool that can help us feel more human in our workplaces.
We learned from social service providers about the wide range of tasks they handle on a daily basis: some are administrative and bureaucratic in nature, while others are more personal and relational. Overall, social service providers want to focus on the relational side of the spectrum, with more time to engage with their patients. We believe that thoughtful integration of AI can help enable this shift.

SSPs want to focus on the relational elements of their job. Thoughtful integration of AI can help them do this.


